Bone regeneration after tumor removal presents a unique set of clinical challenges that demand innovative solutions. Following resection of malignant or benign tumors, patients often face large bone defects that impair structural integrity and function. Research in orthopedics and regenerative medicine focuses on restoring bone through advanced techniques, combining principles of osteogenesis, angiogenesis, and smart materials. This article explores the underlying biology, current therapeutic strategies, and emerging technologies poised to transform post‐tumor bone reconstruction.
Pathophysiology of Bone Defects Following Tumor Resection
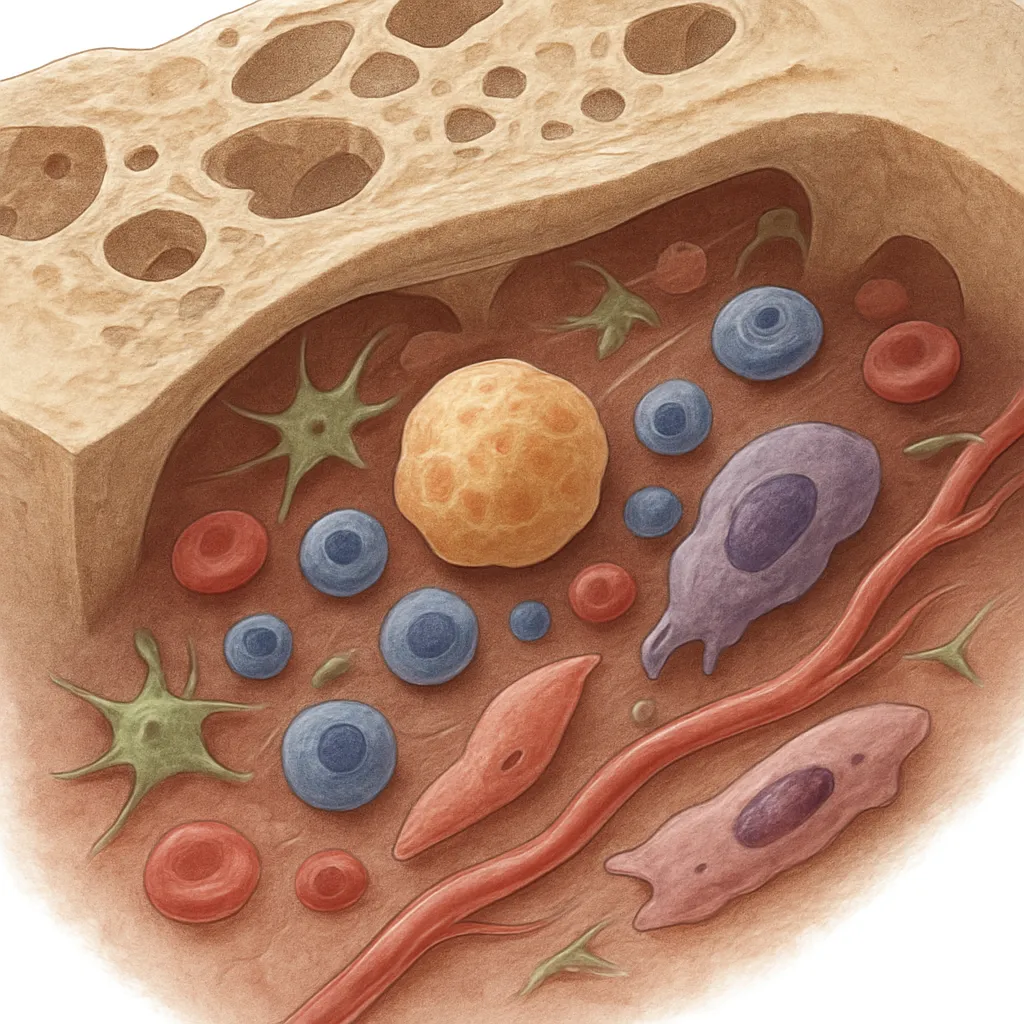
Surgical removal of bone tumors often necessitates wide excision margins to ensure complete eradication of malignant cells. While this approach maximizes oncologic safety, it frequently results in critical‐sized defects that exceed the bone’s natural capacity for self‐repair. Key processes affected include:
- Osteoclasts and osteoblast activity imbalance: Resection alters the remodeling unit, leading to impaired bone turnover.
- Disruption of local vascular networks: Loss of blood supply compromises nutrient delivery, hindering angiogenesis.
- Damage to periosteal stem cell niches: The periosteum contains precursors essential for chondrogenesis and direct ossification.
Without adequate intervention, these defects can progress to nonunion, chronic pain, and functional disability. Understanding the microenvironment post‐resection is crucial for designing targeted therapies that support innate healing while minimizing complications.
Current Strategies for Bone Regeneration
Clinicians employ a range of techniques to address post‐tumor bone defects. These methods vary in complexity, risk profile, and potential for full functional recovery.
Autologous and Allogeneic Grafts
Harvesting bone from the patient (autograft) remains the gold standard due to its intrinsic osteogenic cells, osteoinductive proteins, and native matrix. However, donor site morbidity and limited graft volume pose challenges. Allografts offer larger volumes but carry risks of immune rejection and disease transmission.
- Autografts: Strong osteogenesis potential but donor site complications.
- Allografts: Readily available bulk grafts, require processing to reduce immunogenicity.
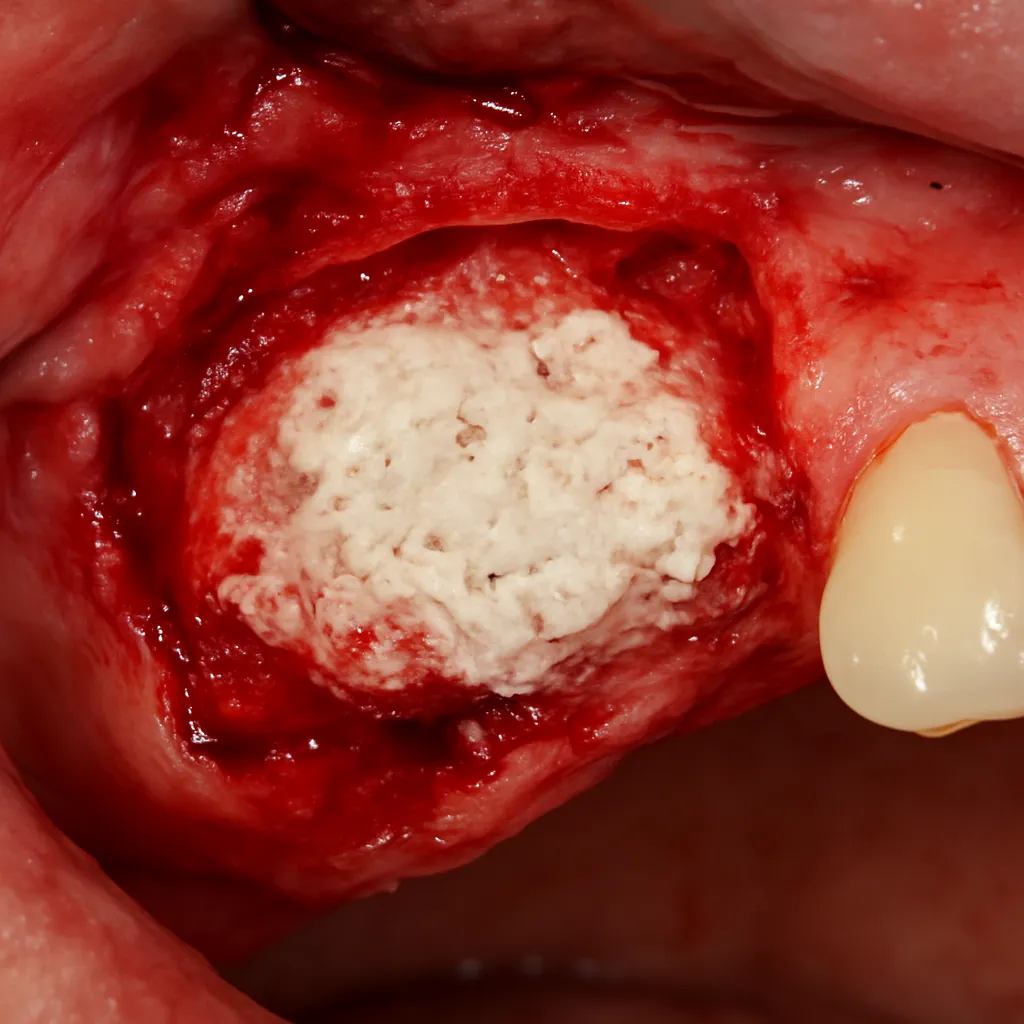
Synthetic and Composite Biomaterials
Synthetic scaffolds provide customizable solutions for defect filling. Commonly used biomaterials include calcium phosphates (hydroxyapatite, tricalcium phosphate), bioactive glasses, and polymeric matrices (PLGA, PCL). Composite scaffolds combine ceramics with polymers to balance mechanical strength and biodegradability.
- Calcium phosphate ceramics: Mimic bone mineral, support matrix deposition.
- Bioactive glasses: Stimulate local cell activity and form chemical bonds with host bone.
- Polymeric scaffolds: Offer tunable degradation and porosity, allow drug delivery.
Growth Factors and Cellular Therapies
Regenerative strategies often incorporate bioactive molecules and cells to enhance healing. Key elements include:
- Growth factors such as BMP‐2 and BMP‐7: Induce mesenchymal stem cell recruitment and differentiation.
- Mesenchymal stem cells (MSCs): Multipotent cells capable of osteogenic and chondrogenic differentiation.
- Platelet-rich plasma (PRP): Autologous source of cytokines and growth factors that modulate inflammation and tissue repair.
Combining MSCs with growth factors on a scaffold can create an osteoinductive environment that accelerates bone formation, although concerns about dose, delivery method, and cost remain under investigation.
Emerging Technologies and Future Directions
Innovations in tissue engineering and materials science are driving the next wave of therapies designed to overcome limitations of conventional grafts.
Tissue Engineering and 3D Bioprinting
Advances in 3D bioprinting enable fabrication of patient-specific scaffolds that match defect geometry. Techniques involve:
- Layer‐by‐layer deposition of polymers and ceramics to create interconnected pore networks.
- Incorporation of living cells or bioinks loaded with MSCs to produce a living construct.
- Custom design based on CT imaging for precise anatomical fit.
This approach fosters integration with host tissue and optimizes mechanical stability. Early preclinical models have demonstrated promising results in promoting balanced bone formation and vascular ingrowth.
Nanotechnology and Smart Materials
The application of nanotechnology is revolutionizing scaffold design at the molecular level. Key developments include:
- Nanostructured surfaces that mimic the natural extracellular matrix, enhancing cell adhesion and proliferation.
- Controlled release systems: Nanocarriers deliver growth factors or genes in a sustained manner.
- Stimuli‐responsive materials: Polymers that alter properties in response to pH, temperature, or mechanical load, enabling on‐demand therapeutic action.
Smart implants capable of sensing local biochemical changes and releasing therapeutics accordingly could significantly improve outcomes, especially in long‐term tumor surveillance where recurrence risk exists.
Regulatory and Clinical Considerations
Bringing novel regenerative solutions to the clinic involves rigorous testing and regulatory approval. Important considerations include:
- Safety and biocompatibility: Ensuring no adverse immune reactions or toxicity from new materials.
- Efficacy in large animal models: Demonstrating functional recovery and mechanical integration under physiological loads.
- Scalability and manufacturing: Developing cost‐effective processes for mass production without compromising quality.
Collaborations between surgeons, engineers, and regulatory experts streamline translation from bench to bedside, ultimately benefiting patients who require reliable bone reconstruction after tumor surgery.