Bone necrosis of the jaw represents a serious complication that can arise from various medical treatments and systemic conditions. This condition, often referred to as medication-related osteonecrosis of the jaw (MRONJ), has gained significant attention due to its impact on patient quality of life and the challenges it poses for clinicians. An understanding of the underlying pathophysiology, risk factors, diagnostic approaches, and management strategies is crucial for effective prevention and therapy.
Pathophysiology of Jaw Bone Necrosis
The development of necrotic bone tissue in the jaw involves a complex interplay between impaired bone remodeling, reduced vascular supply, and local microbial invasion. Under normal circumstances, bone homeostasis is maintained through a balance between osteoclastic resorption and osteoblastic formation. When antiresorptive agents, such as bisphosphonates or denosumab, disrupt this equilibrium, bone turnover decreases, leading to areas of weak or nonviable bone.
Cellular Mechanisms
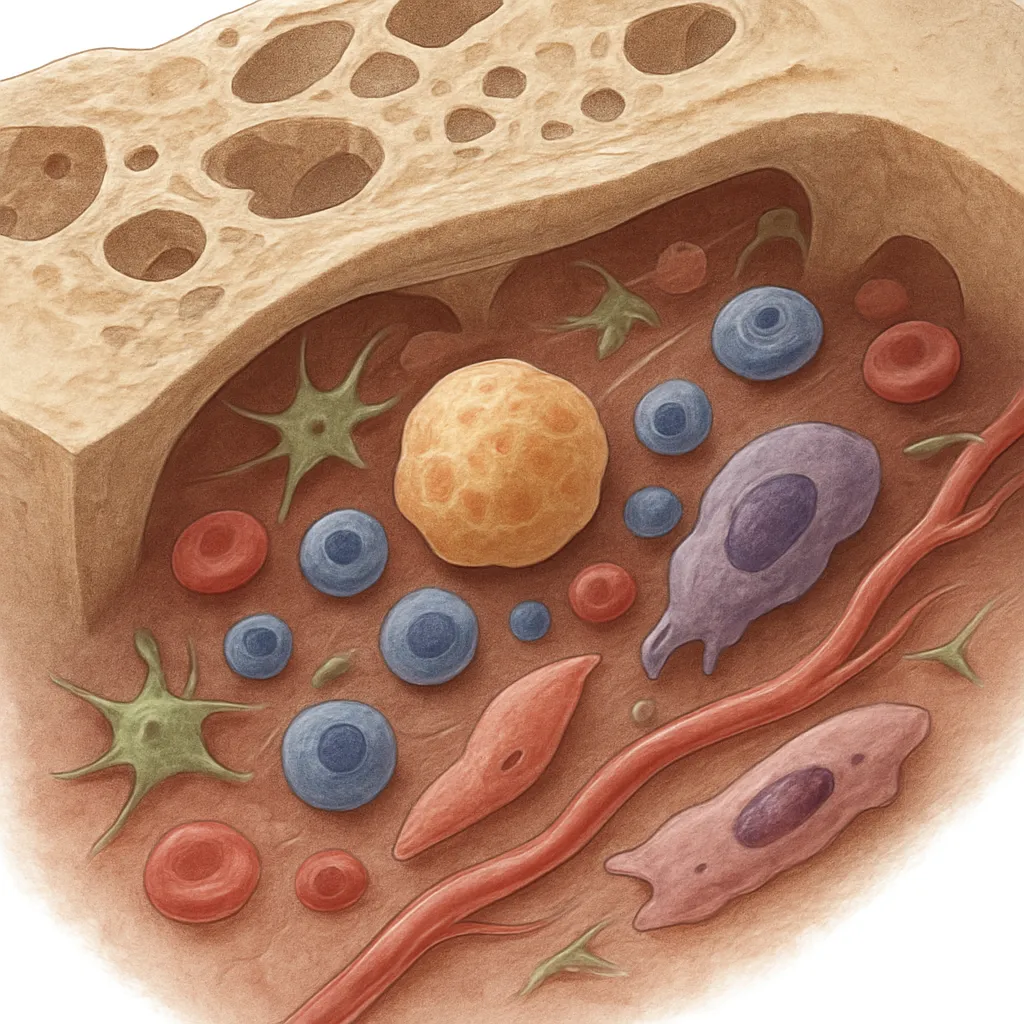
Osteoclast inhibition, coupled with suppressed angiogenesis, results in decreased new blood vessel formation. The reduced perfusion exacerbates hypoxia, contributing to cell death and accumulation of microdamage. In the jaw, high bone turnover due to constant mechanical stress makes it particularly susceptible to these effects. Additionally, soft tissue injury or dental procedures can expose the bone, allowing opportunistic pathogens to colonize and form biofilms.
Role of Inflammation and Immunity
Chronic inflammation further compromises bone integrity. Pro-inflammatory cytokines, such as TNF-α and IL-6, stimulate osteoclast activity outside the normal remodeling cycle, creating localized areas of necrotic bone. At the same time, immune suppression—whether due to systemic disease, chemotherapy, or corticosteroid use—impairs the body’s ability to clear infection and repair damaged tissue.
Risk Factors and Etiology
Several factors converge to increase the risk of jaw necrosis. Recognizing these elements allows clinicians to stratify patients and implement preventive measures.
- Antiresorptive medications: Long-term use of bisphosphonates and denosumab is the primary contributor to MRONJ.
- Antiangiogenic therapies: Agents targeting VEGF pathways reduce blood supply to bony structures.
- Systemic diseases: Diabetes mellitus and autoimmune disorders impair wound healing and immune response.
- Corticosteroid therapy: Prolonged glucocorticoid use increases susceptibility to infection and delays tissue regeneration.
- Local triggers: Dental extractions, implant placement, and ill-fitting dentures can breach mucosal barriers.
While osteoporosis patients receiving low-dose therapy carry a lower risk compared to oncology patients on high-dose regimens, clinicians must remain vigilant regardless of indication.
Clinical Presentation and Diagnosis
Early recognition of jaw necrosis is essential to prevent progression. Symptoms may range from mild discomfort to severe pain and pathological fracture.
Signs and Symptoms
- Exposed bone in the oral cavity lasting more than eight weeks
- Localized and sometimes radiating pain
- Soft tissue swelling and erythema
- Fistula formation or purulent drainage
- Altered sensation due to nerve involvement
Diagnostic Imaging
Panoramic radiographs can reveal osteolytic areas, sclerotic bone, or sequestra. Cone-beam computed tomography (CBCT) provides higher resolution of cortical disruption and periosteal reactions. In certain cases, magnetic resonance imaging (MRI) may be used to assess soft tissue extension and vascularity.
Biopsy and Microbiology
When clinical and imaging findings are inconclusive, a small bone biopsy can confirm necrosis by demonstrating empty lacunae and bacteria-laden biofilm. Culture and sensitivity testing guide antimicrobial therapy.
Management Strategies
Treatment of jaw necrosis is multifaceted, focusing on pain control, infection eradication, and promotion of bone healing.
Conservative Approaches
- Antimicrobial rinses (e.g., chlorhexidine)
- Systemic antibiotics targeting oral flora, such as penicillin or clindamycin
- Analgesics to manage pain
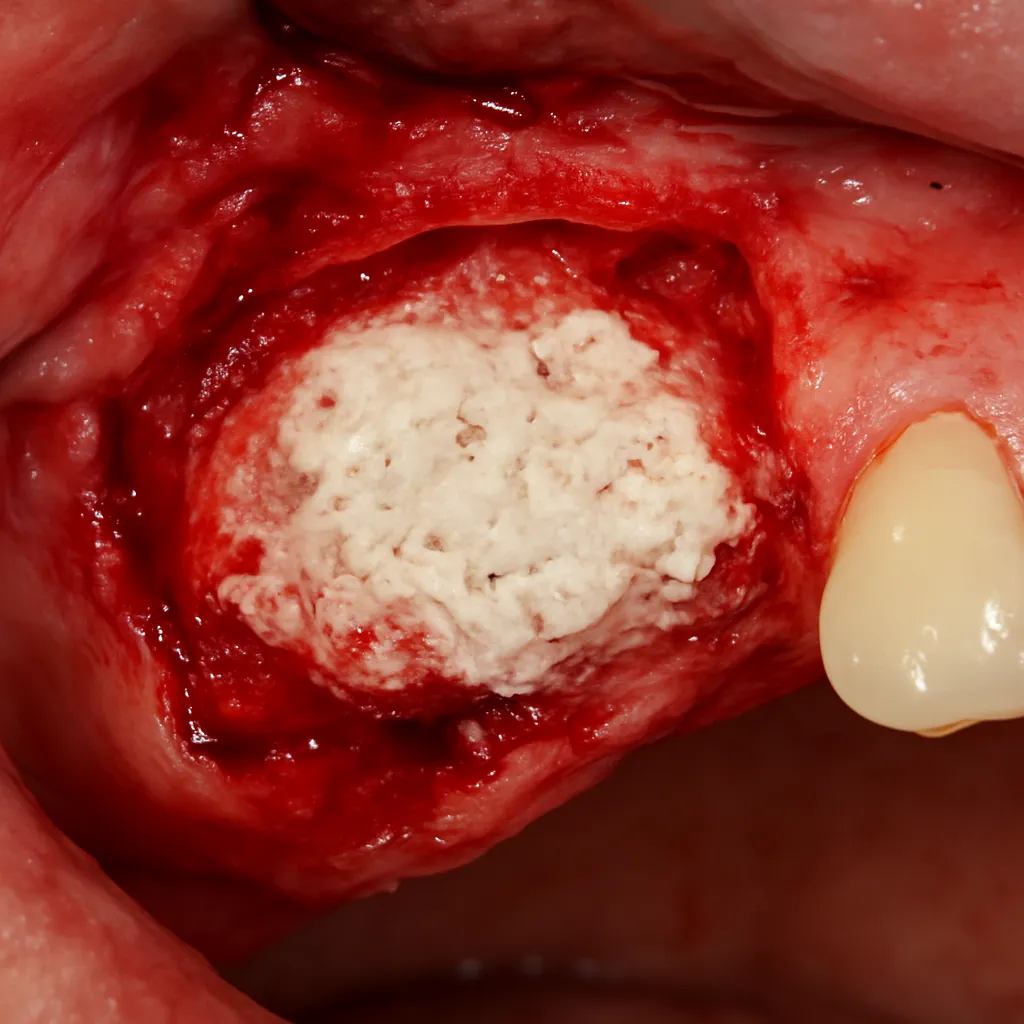
- Minimally invasive debridement to remove loose sequestra
Surgical Intervention
Reserved for advanced cases, resection of necrotic segments followed by primary closure or local flap coverage can promote healing. In extensive defects, microvascular free flaps may reconstruct the mandible, restoring both function and aesthetics.
Modification of Medical Therapy
Collaboration with the patient’s primary physician or oncologist is critical. A drug “holiday” from antiresorptive agents may be considered, though the decision should weigh fracture risk against jaw healing potential. It is important to note that stopping medication does not guarantee rapid reversal of necrotic changes due to the long half-life of bisphosphonates in bone.
Emerging Therapies and Future Directions
Innovations in the treatment of jaw necrosis aim to enhance bone regeneration and reduce morbidity. Recent studies have explored:
- Low-level laser therapy (LLLT) to stimulate cellular proliferation and angiogenesis
- Platelet-rich fibrin (PRF) adjuncts to deliver growth factors directly to the surgical site
- Local administration of teriparatide to promote new bone formation
- Stem cell therapy leveraging mesenchymal stem cells for targeted repair
The integration of these techniques into clinical practice requires robust randomized controlled trials. Meanwhile, emphasis on early risk assessment, patient education, and meticulous oral care remains the cornerstone of prevention.