The complex relationship between **obesity** and **bone** health has garnered substantial attention in recent years. While excessive body weight was once believed to confer protective effects on the **skeletal** system by increasing mechanical loading, emerging evidence suggests that adiposity may exert detrimental influences on **bone quality** and fracture risk. This article explores multiple dimensions of this interaction, addressing clinical, cellular, and molecular aspects that shape our understanding of how **excess fat** affects the integrity and function of bone tissue.
Etiology and Pathophysiology of Obesity-Related Bone Alterations
Obesity is characterized by an increased accumulation of **adipose tissue**, chronic low-grade **inflammation**, and metabolic dysregulation. These factors converge to disrupt normal bone remodeling, a tightly regulated process governed by the activities of **osteoblasts** (bone-forming cells) and osteoclasts (bone-resorbing cells).
Adipokines and Inflammatory Mediators
Adipose tissue secretes a variety of bioactive molecules—collectively known as **adipokines**—including leptin, adiponectin, resistin, and visfatin. Elevated levels of pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6) are hallmarks of obesity. These mediators:
- Promote osteoclastogenesis by upregulating RANKL (Receptor Activator of Nuclear Factor κB Ligand).
- Inhibit osteoblast differentiation and function by antagonizing Wnt/β-catenin signaling.
- Impair bone **matrix** quality by increasing oxidative stress within the bone microenvironment.
Mechanical Loading Versus Fat Mass
Traditional biomechanics posited that higher body weight increases mechanical strain on bone, thus stimulating bone formation and augmenting **bone mineral density**. However, the composition of body mass matters. Excessive fat mass often coexists with reduced lean mass and sarcopenia, which can lead to:
- Altered gait and balance issues, increasing **fall risk**.
- Less effective mechanical loading relative to lean mass contributions.
- Redistribution of marrow adiposity, compromising the niche for skeletal stem cells.
Impact on Bone Mineral Density and Microarchitecture
Studies employing dual-energy X-ray absorptiometry (DXA) and high-resolution peripheral quantitative computed tomography (HR-pQCT) have revealed nuanced effects of obesity on bone density and **microarchitecture**. While DXA often reports normal or increased areal bone mineral density (aBMD) in obese individuals, HR-pQCT data suggest compromised structural integrity.
Trabecular and Cortical Changes
- Trabecular bone: Reduced trabecular thickness and number, leading to greater separation and increased risk of microfractures.
- Cortical bone: Elevated cortical porosity and diminished cortical thickness, weakening the outer shell of long bones and vertebrae.
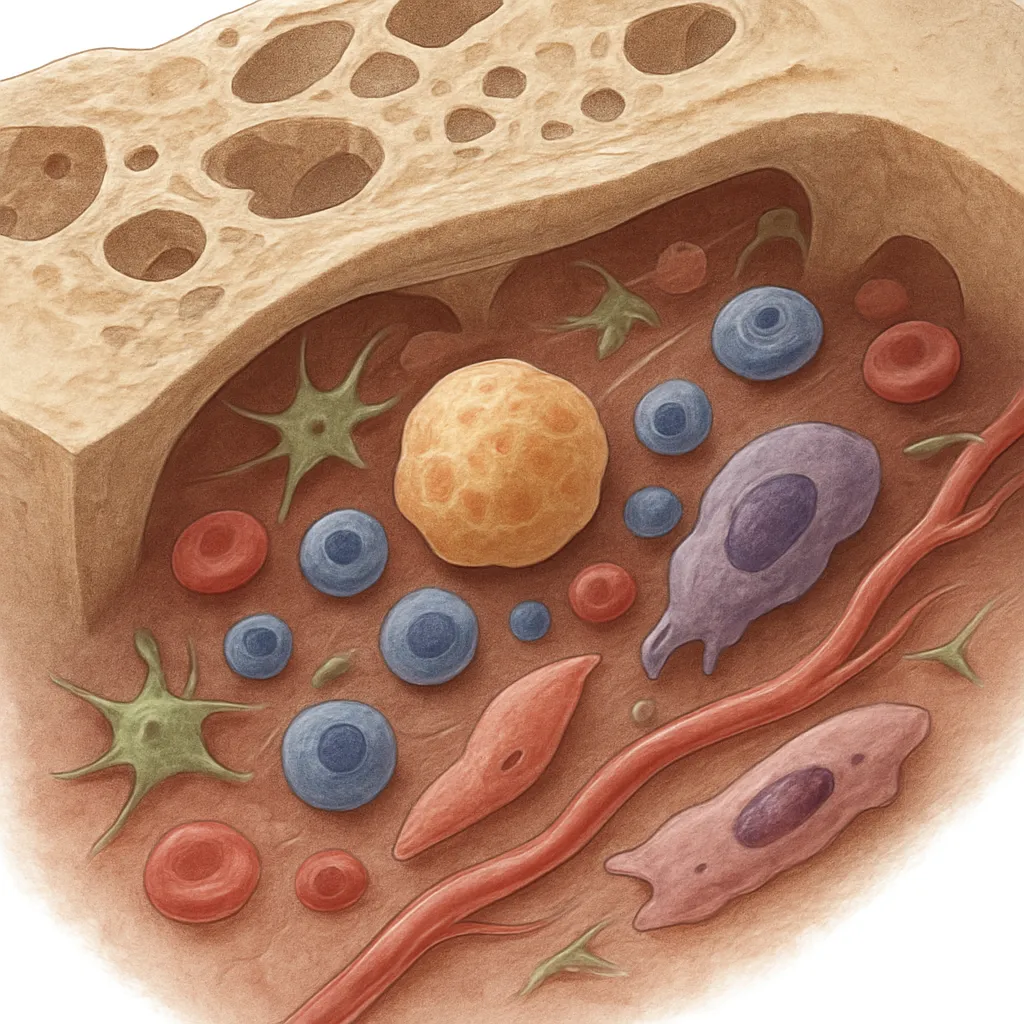
Marrow Adiposity and Hematopoietic Interplay
Bone marrow is not merely a cavity for hematopoiesis but also a site for mesenchymal stem cell (MSC) differentiation. In obesity:
- MSCs preferentially differentiate into adipocytes rather than osteoblasts.
- Increased marrow adipose tissue (MAT) correlates with lower bone formation markers.
- MAT expansion may displace hematopoietic precursors, potentially affecting immune and regenerative functions.
Cellular Mechanisms and Signaling Pathways
A deeper understanding of **cell signaling** has illuminated how obesity-induced factors impair bone remodeling. Key pathways influenced by excessive adiposity include:
Wnt/β-Catenin Signaling Disruption
Wnt ligands bind to Frizzled receptors and LRP5/6 co-receptors on osteoblast progenitors, stabilizing β-catenin and promoting bone formation. In obese states, secreted antagonists such as sclerostin and DKK1 are upregulated, leading to:
- Reduced osteoblast proliferation and survival.
- Lower expression of osteogenic genes (e.g., **RUNX2**, Osterix).
RANK/RANKL/OPG Axis Modulation
The balance between receptor activator of nuclear factor κB ligand (RANKL) and its decoy receptor osteoprotegerin (OPG) is critical for osteoclastogenesis. Obesity shifts this balance by:
- Increasing RANKL production from adipose and bone marrow stromal cells.
- Decreasing OPG synthesis, allowing enhanced osteoclast activity.
Insulin, IGF-1, and Metabolic Hormones
Hyperinsulinemia and insulin resistance alter bone cell metabolism. Although insulin exerts anabolic effects on osteoblasts, chronic insulin resistance is associated with:
- Dysregulated IGF-1 signaling, a potent stimulator of osteoblast proliferation.
- Increased advanced glycation end products (AGEs), which stiffen the collagen matrix and impair bone toughness.
Clinical Implications and Diagnostic Biomarkers
Recognizing obesity as a risk factor for poor bone quality necessitates refined clinical approaches to assessment, prevention, and management.
Fracture Risk Assessment
Tools like FRAX may underestimate fracture risk in obese patients due to reliance on aBMD and traditional risk factors. Considerations include:
- Integration of trabecular bone score (TBS) to evaluate microarchitectural deterioration.
- Assessment of muscle strength and balance to gauge fall risk.
- Inclusion of adiposity measures (e.g., waist circumference, body composition analysis).
Biomarkers of Bone Turnover
Monitoring serum and urine markers offers insight into dynamic changes in bone remodeling:
- Formation markers: osteocalcin, procollagen type I N-terminal propeptide (PINP).
- Resorption markers: C-terminal telopeptide of type I collagen (CTX), N-terminal telopeptide (NTX).
- Inflammatory markers: high-sensitivity C-reactive protein (hs-CRP), IL-6.
Therapeutic Interventions
Combating the negative impact of obesity on bone health involves multifaceted strategies:
- Lifestyle modifications: weight reduction through calorie restriction, combined with resistance and weight-bearing exercise to preserve **lean mass** and stimulate bone formation.
- Pharmacotherapy: bisphosphonates and denosumab may help reduce resorption, while anabolic agents such as teriparatide can promote bone formation.
- Emerging therapies: modulators of Wnt signaling and adipokine-targeting agents are in development to restore healthy coupling of osteoblast and osteoclast activities.
Future Directions in Research
To effectively unravel the interplay between obesity and **bone integrity**, future studies should focus on:
- Longitudinal cohort analyses integrating genetic, metabolic, and imaging data.
- Advanced imaging modalities such as high-field MRI for noninvasive assessment of marrow adiposity.
- Identification of novel **biomarkers** that reflect functional aspects of bone quality beyond density.
- Precision medicine approaches to tailor interventions based on individual metabolic and skeletal profiles.
This evolving field underscores the need to view obesity not only as a metabolic disorder but also as a condition with profound skeletal consequences. A comprehensive approach that addresses both adipose-driven metabolic dysfunction and skeletal fragility will be critical to improving bone health outcomes in the growing obese population.