Bone remodeling after injury represents a finely tuned interplay of cellular activities, growth factors, and mechanical cues. This article examines the processes by which bone tissue detects damage, initiates repair, and restores structural integrity. By exploring the roles of critical cell types, signaling pathways, and emerging technologies, readers will gain a comprehensive understanding of how skeletal tissue adapts and heals.
Overview of Bone Remodeling Processes
The skeletal system remains in a state of dynamic equilibrium, continuously resorbing and forming bone to maintain strength, mineral homeostasis, and structural integrity. When an injury such as a fracture occurs, the balance tips toward repair. Three overlapping phases—
- Inflammation
- Repair and callus formation
- Remodeling
guide the restoration of normal bone architecture. Each phase involves specialized cell types and molecular signals that coordinate the sequence of events from hematoma development to eventual reestablishment of the original bone shape and mechanical competence.
Inflammatory Phase
The initial inflammatory response recruits immune cells to the injury site. Neutrophils and macrophages clear debris and secrete cytokines such as interleukin-1 (IL-1) and tumor necrosis factor-alpha (TNF-α). These mediators create a microenvironment that primes mesenchymal progenitors for subsequent differentiation.
Repair Phase
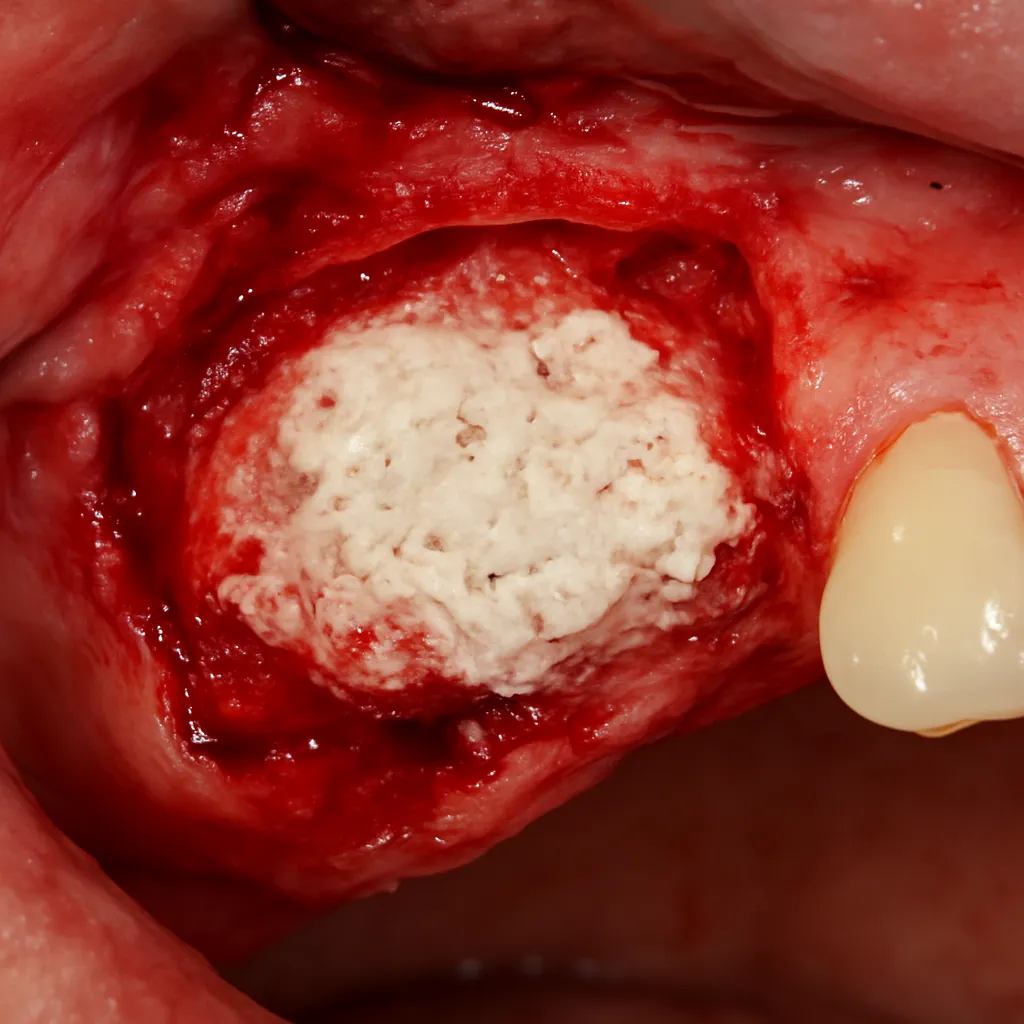
During repair, undifferentiated cells migrate to the fracture gap and form a soft callus composed of collagen and cartilage. Vascular invasion follows, facilitating the deposition of a bony callus by newly differentiated osteoblasts. This provisional matrix stabilizes the fracture and provides a scaffold for further remodeling.
Remodeling Phase
The last phase involves the coordinated actions of osteoclasts and osteoblasts. Osteoclasts resorb the excess callus, while osteoblasts fill resorption cavities with lamellar bone. This continuous cycle restores the bone’s original shape, microarchitecture, and load-bearing capabilities.
Cellular and Molecular Mechanisms
Bone remodeling hinges on the interplay between two principal cell types: the bone-resorbing osteoclasts and the bone-forming osteoblasts. Both arise from distinct progenitor lineages and are regulated by a balance of local factors and systemic hormones.
Osteoclast Differentiation and Function
Osteoclasts originate from hematopoietic stem cells in the bone marrow. Under the influence of macrophage colony-stimulating factor (M-CSF) and receptor activator of nuclear factor kappa-Β ligand (RANKL), mononuclear precursors fuse to form multinucleated cells capable of resorbing mineralized matrix. The enzymatic machinery, including tartrate-resistant acid phosphatase (TRAP) and cathepsin K, degrades both the organic and inorganic components of bone.
Osteoblast Lineage and Matrix Production
Osteoblasts derive from mesenchymal stem cells. Key transcription factors such as Runx2 and osterix drive commitment to the osteogenic lineage. These cells secrete type I collagen and non-collagenous proteins like osteocalcin and osteopontin, forming the organic framework of the bone matrix. Mineralization then occurs through the deposition of hydroxyapatite crystals.
RANK/RANKL/OPG Axis
The RANK/RANKL/osteoprotegerin (OPG) signaling axis serves as a critical switch controlling osteoclast activity. RANKL, expressed by osteoblasts and stromal cells, binds to RANK on osteoclast precursors, promoting their differentiation. OPG, a decoy receptor produced by osteoblasts, sequesters RANKL, thereby inhibiting excessive resorption and maintaining skeletal homeostasis.
Mechanical and Biochemical Signaling
Bone is a mechanosensitive tissue that translates physical forces into molecular responses—a process termed mechanotransduction. Microdamage from mechanical loading or injury triggers localized remodeling to reinforce stressed regions.
Integrin-Mediated Mechanosensing
Integrins on osteoblast and osteocyte surfaces detect changes in extracellular matrix tension. Activation of focal adhesion kinase (FAK) and downstream pathways, including MAPK and PI3K/Akt, stimulate gene expression profiles that enhance matrix production and inhibit apoptosis.
Wnt/β-Catenin Pathway
The Wnt signaling cascade promotes osteoblast proliferation and survival. Binding of Wnt ligands to Frizzled receptors stabilizes β-catenin, allowing its nuclear translocation to activate osteogenic genes. Dysregulation of this pathway can lead to impaired bone formation or pathological overgrowth.
Growth Factors and Cytokines
Multiple autocrine and paracrine factors regulate repair:
- Transforming Growth Factor-beta (TGF-β): Stimulates fibroblast proliferation and collagen synthesis.
- Bone Morphogenetic Proteins (BMPs): Induce chondrogenesis and osteogenesis.
- Insulin-like Growth Factors (IGFs): Enhance osteoblast survival and matrix deposition.
Clinical Implications and Therapeutic Strategies
Understanding the molecular basis of bone remodeling paves the way for novel treatments to improve fracture healing and combat metabolic bone diseases such as osteoporosis.
Pharmacological Interventions
- Bisphosphonates: Inhibit osteoclast activity by inducing apoptosis and disrupting resorption lacunae.
- Denosumab: A monoclonal antibody against RANKL, reducing bone turnover.
- Teriparatide: Recombinant parathyroid hormone analog that stimulates osteoblast function when administered intermittently.
Biomaterials and Scaffolds
Advancements in bioceramic and polymer-based scaffolds provide osteoconductive frameworks for cell attachment and proliferation. Incorporation of growth factors or stem cells into these matrices enhances local regeneration and accelerates bridging of critical-size defects.
Cell-Based Therapies
Mesenchymal stem cell transplantation offers a strategy to augment endogenous repair. Harvested from bone marrow or adipose tissue, these multipotent cells can be preconditioned to express osteogenic markers before implantation into injury sites.
Emerging Technologies in Bone Regeneration
Recent innovations harness the power of tissue engineering, gene therapy, and advanced imaging to refine our approach to skeletal repair.
3D Bioprinting
Layer-by-layer fabrication of patient-specific grafts using bioinks composed of hydrogels and live cells shows promise for complex defect reconstruction. This technique allows precise spatial patterning of multiple cell types and growth factors to mimic native bone architecture.
CRISPR/Cas9-Mediated Gene Editing
Targeted modification of genes involved in osteogenesis or inflammation can enhance the regenerative potential of transplanted cells. Editing strategies focus on upregulating pro-osteogenic factors or downregulating inhibitors of matrix formation.
Advanced Imaging and Monitoring
High-resolution micro-CT and molecular imaging agents enable noninvasive tracking of callus formation, vascular ingrowth, and scaffold integration. These tools facilitate real-time assessment of therapeutic efficacy and guide personalized treatment adjustments.