Antiresorptive drugs represent a cornerstone in the management of metabolic bone diseases by targeting the cellular processes responsible for bone breakdown. Through inhibition of osteoclast activity and modulation of bone turnover, these therapies help maintain skeletal strength, reduce fracture risk, and restore balanced calcium homeostasis. Understanding their mechanisms, clinical applications, and safety profiles is essential for optimizing patient outcomes in conditions such as osteoporosis and other high-turnover bone disorders.
Mechanisms of bone remodeling and cellular targets
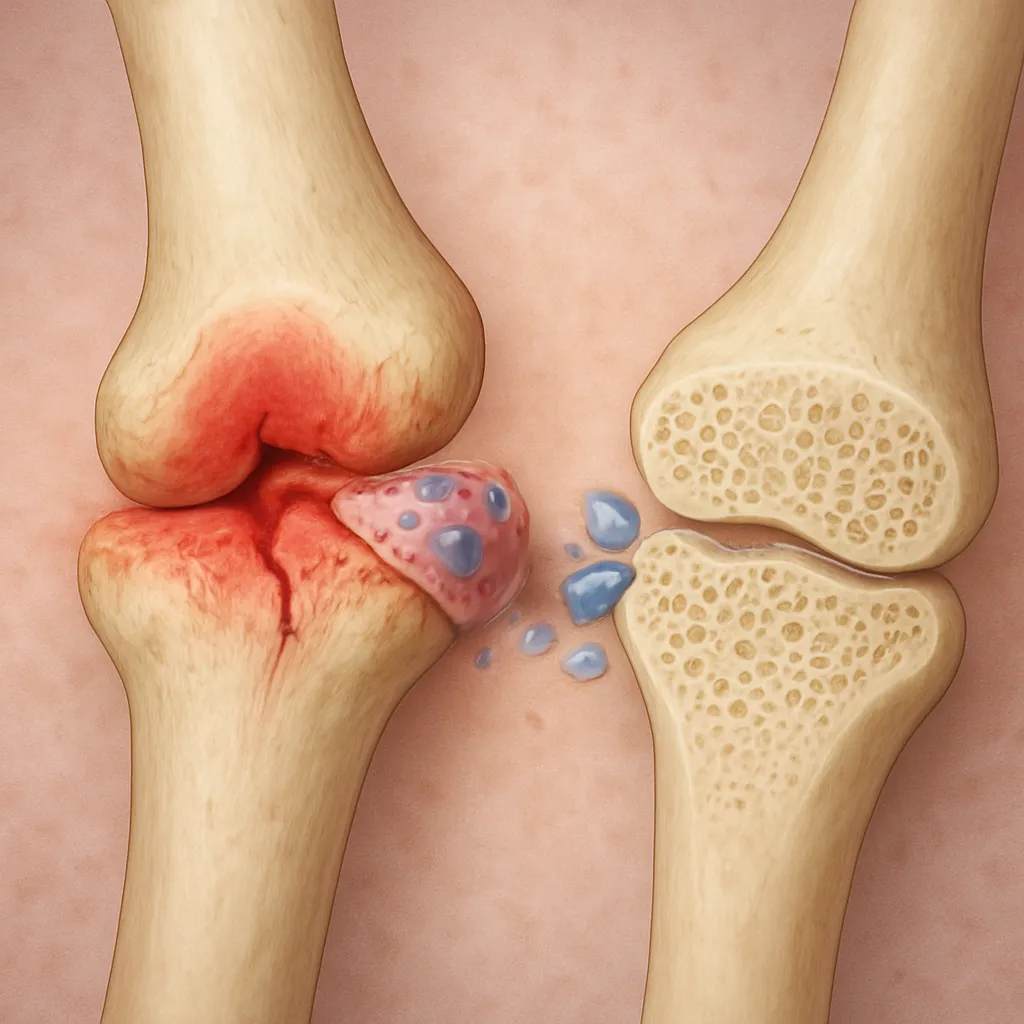
Bone tissue undergoes constant renewal via a tightly regulated cycle involving resorption by osteoclasts and formation by osteoblasts. This dynamic process, known as bone remodeling, ensures structural integrity and adaptation to mechanical stress. In healthy adults, resorption and formation are coupled; however, imbalances can lead to weakened bone architecture and increased susceptibility to fractures.
Osteoclast differentiation and activation
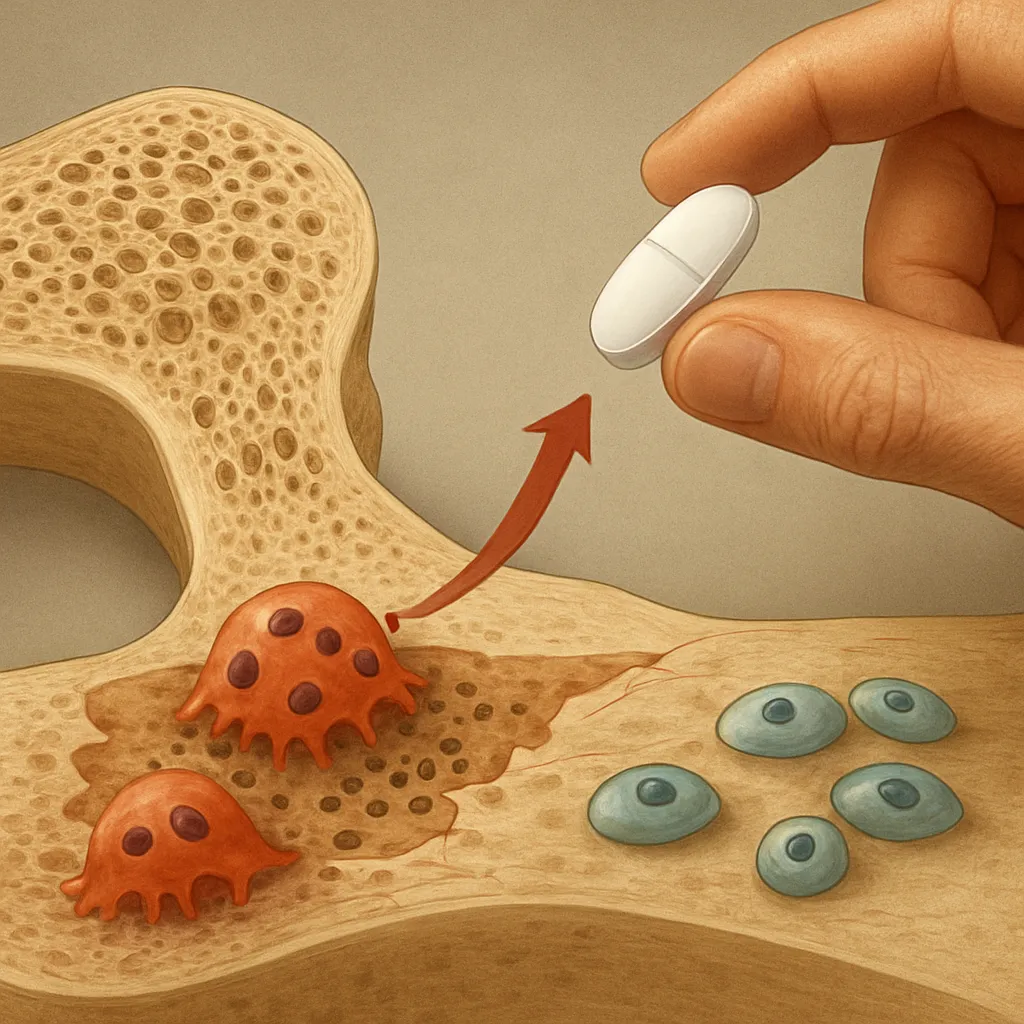
Derived from hematopoietic precursors, osteoclasts attach to bone surfaces, secrete acidic protons and proteolytic enzymes, and dissolve the mineral and collagen matrix. Key cytokines such as RANKL (Receptor Activator of Nuclear factor Kappa-Β Ligand) and M-CSF (Macrophage Colony-Stimulating Factor) govern osteoclastogenesis. Antiresorptive agents disrupt these signaling pathways, thereby reducing the number and activity of osteoclasts.
Osteoblast-osteoclast coupling
Osteoblasts not only synthesize new bone but also regulate osteoclast formation through the secretion of RANKL and osteoprotegerin (OPG). Therapeutics that enhance OPG or inhibit RANKL shift the balance towards bone formation. By modulating cellular crosstalk, antiresorptive drugs indirectly affect osteoblasts, promoting a healthier remodeling cycle.
Classes of antiresorptive agents and pharmacodynamics
Several drug classes have been developed to curb excessive bone resorption. Their diverse molecular structures and modes of action allow tailored treatment strategies based on patient-specific factors.
- Bisphosphonates: These pyrophosphate analogues bind avidly to hydroxyapatite in bone. When osteoclasts attempt resorption, bisphosphonates impair their cytoskeleton and induce apoptosis. Common agents include alendronate, risedronate, ibandronate, and zoledronic acid.
- Denosumab: A fully human monoclonal antibody targeting RANKL. By neutralizing RANKL, denosumab prevents receptor activation on osteoclast precursors, sharply reducing osteoclast formation and activity.
- Selective Estrogen Receptor Modulators (SERMs): Agents such as raloxifene mimic estrogen’s protective effects on bone without stimulating breast or uterine tissue.
- Calcitonin: A hormone that binds to specific receptors on osteoclasts, inhibiting their function and providing modest antiresorptive effects.
Pharmacokinetic considerations
Bisphosphonates exhibit low oral bioavailability and require fasting administration, whereas denosumab is delivered subcutaneously every six months. The prolonged skeletal retention of bisphosphonates contrasts with the reversible action of denosumab, influencing rebound bone turnover upon discontinuation.
Clinical applications and safety considerations
Antiresorptive therapies are indicated in a variety of settings:
- Osteoporosis: Postmenopausal and glucocorticoid-induced cases benefit from fracture prevention.
- Bone metastases: Reduction of skeletal-related events in malignancies such as breast and prostate cancer.
- Paget’s disease: Alleviation of bone pain and deformities by normalizing excessive remodeling.
- Hypercalcemia of malignancy: Rapid correction of elevated serum calcium levels.
Monitoring treatment efficacy
Bone mineral density (BMD) assessments and biochemical markers of bone turnover guide therapy adjustments. Successful antiresorptive treatment typically yields increased BMD and decreased resorption markers (e.g., CTX, NTX).
Adverse effects and risk mitigation
Although generally well tolerated, potent inhibition of bone resorption may lead to rare but serious events:
- Osteonecrosis of the jaw (osteonecrosis): Most commonly seen in cancer patients receiving high-dose bisphosphonates or denosumab. Dental evaluation prior to therapy can minimize risk.
- Atypical femoral fractures: Associated with prolonged bisphosphonate use; drug holidays after 5 years of therapy are considered for low-risk individuals.
- Hypocalcemia: Ensure adequate vitamin D and calcium supplementation, especially when initiating denosumab.
Emerging strategies and future perspectives
Research continues to explore novel antiresorptive targets and optimize existing treatments:
- Cathepsin K inhibitors aim to selectively block osteoclast collagenase activity without affecting survival.
- Combination therapies pairing antiresorptives with anabolic agents seek to maximize bone strength.
- Biomaterials and targeted drug delivery systems are under investigation to improve site-specific efficacy and reduce systemic exposure.
Advances in genomics and personalized medicine may soon enable clinicians to predict individual responses, refining therapeutic regimens and enhancing overall efficacy in managing bone diseases.