The process of bone repair involves a sophisticated interplay of cellular, molecular, and biochemical events that together restore skeletal integrity after injury. Clinicians and researchers increasingly rely on specialized indicators to assess healing progression and tailor therapeutic strategies. This article explores the fundamental stages of bone repair, examines pivotal biomarkers, and discusses how these markers inform clinical decision-making and future research directions.
Bone Healing Physiology and Stages
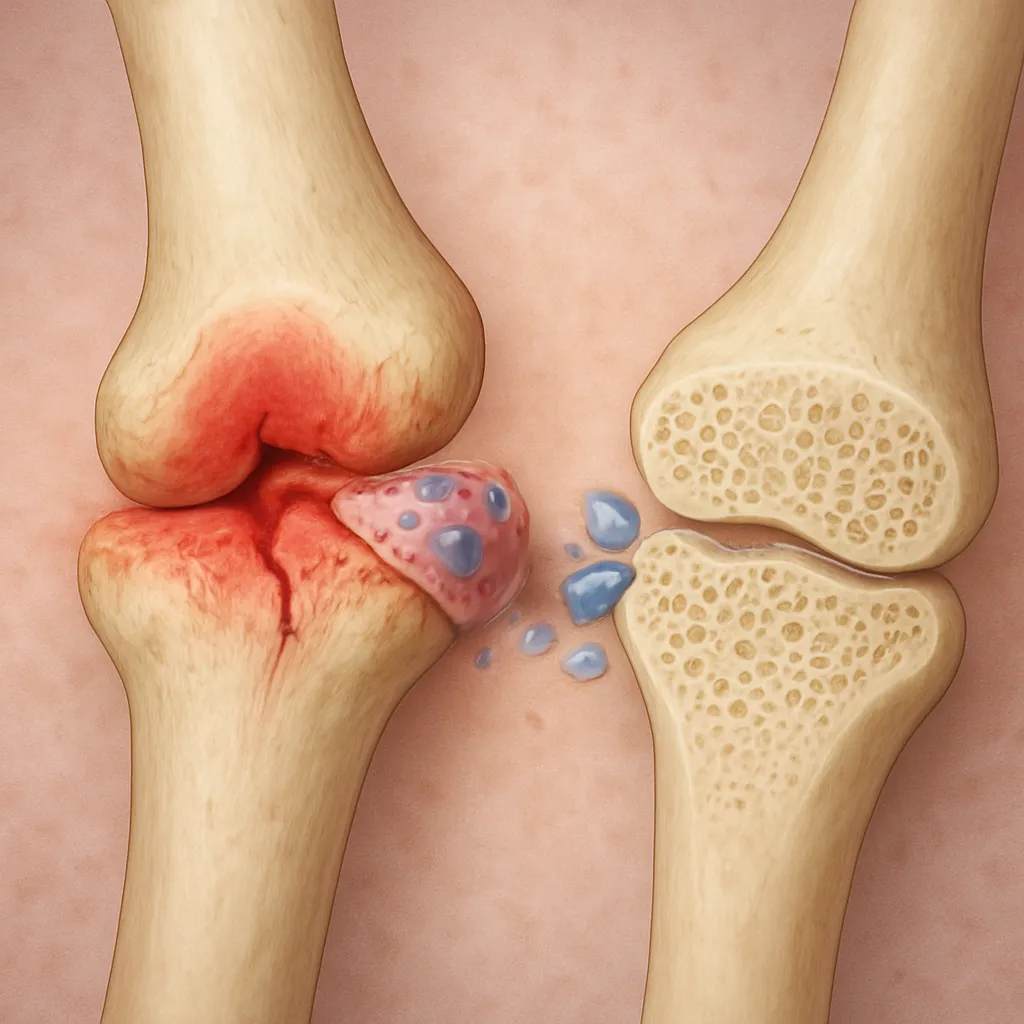
Inflammatory Phase
The first stage in fracture healing is marked by a controlled inflammatory response. Within hours of injury, blood vessels rupture and form a hematoma at the fracture site. This clot provides a scaffold for invading inflammatory cells, including neutrophils and macrophages, which release cytokines such as interleukin-1 (IL-1) and tumor necrosis factor-alpha (TNF-α). These signaling molecules recruit mesenchymal stem cells (MSCs) and promote angiogenesis. The careful balance between pro-inflammatory and anti-inflammatory signals is crucial for preventing chronic inflammation and ensuring timely progression to the reparative phase.
Reparative Phase
As inflammation subsides, MSCs differentiate into chondrocytes and osteoblasts, forming a soft callus composed of cartilage and fibrovascular tissue. Gradually, this provisional matrix undergoes endochondral ossification, where chondrocytes produce collagen type II and secrete factors that trigger mineral deposition. Osteoblasts subsequently lay down a woven bone matrix rich in type I collagen. This stage relies on growth factors such as bone morphogenetic proteins (BMPs) and transforming growth factor-beta (TGF-β) to orchestrate cellular proliferation and matrix synthesis.
Remodeling Phase
The final stage transforms the mechanically inferior woven bone into lamellar bone with restored biomechanical strength. Osteoclasts resorb excess bone while osteoblasts continue to deposit organized lamellae aligned along stress lines. This process of bone remodeling can last for months to years, ultimately reestablishing the original bone contour and internal structure. Hormonal regulators such as parathyroid hormone (PTH) and calcitonin modulate the coupling between resorption and formation, ensuring skeletal homeostasis.
Key Biomarkers in Bone Healing
Cytokines and Growth Factors
These soluble mediators are essential for intercellular communication during bone repair. Measuring serum or local concentrations of cytokines (e.g., IL-6, IL-10) and growth factors (e.g., VEGF, BMP-2) helps determine the inflammatory state and angiogenic potential of the healing tissue. Elevated IL-6 levels in early healing correlate with increased callus volume, while persistent high TNF-α may indicate risk of non-union. Advances in multiplex assays allow simultaneous detection of dozens of cytokines, providing a comprehensive profile of the repair environment.
Bone Formation Markers
Markers of new bone synthesis reflect the activity of osteoblasts and matrix deposition. Commonly used assays include:
- Osteocalcin: A non-collagenous protein secreted by mature osteoblasts, indicative of matrix maturation.
- Bone-specific alkaline phosphatase (BSAP): An enzyme associated with early osteoblast differentiation and matrix mineralization.
- Procollagen type I N-terminal propeptide (PINP): Released during the synthesis of type I collagen, a major component of bone extracellular matrix.
Temporal trends in these markers can forecast the pace of osteogenesis and inform the need for interventions such as bone grafting or osteoinductive therapies.
Bone Resorption Markers
Osteoclast-mediated degradation of mineralized matrix releases several detectable fragments into the circulation and urine. Key indicators include:
- C-terminal telopeptide of type I collagen (CTX): A degradation product reflecting the rate of bone resorption.
- N-terminal telopeptide (NTX): Another collagen breakdown fragment commonly measured in urine samples.
- Tartrate-resistant acid phosphatase 5b (TRACP 5b): An enzyme produced by active osteoclasts.
Monitoring these markers alongside formation indicators provides a window into the coupling efficiency of bone turnover and predicts potential imbalances leading to delayed healing or excessive bone loss.
Diagnostic and Prognostic Applications
Serum and Urinary Biomarker Analysis
Blood and urine tests are minimally invasive methods for assessing biochemical changes during bone repair. Serial measurements allow dynamic monitoring of healing trajectories. Elevated BSAP and PINP within the first month post-fracture often correlate with robust callus formation, while persistently high CTX levels may signal overactive resorption and risk of non-union. Combining biomarkers into a multi-analyte panel enhances sensitivity and specificity compared to single-marker assays.
Imaging and Biomarker Integration
Conventional radiography and advanced imaging modalities such as computed tomography (CT) and magnetic resonance imaging (MRI) remain the gold standards for visualizing structural changes. However, early biochemical alterations often precede radiographic evidence of callus formation. Integrating imaging findings with diagnostic biomarker profiles enables clinicians to:
- Identify patients at risk for delayed healing.
- Optimize rehabilitation protocols based on individual healing rates.
- Adjust pharmacological treatments, including bisphosphonates or PTH analogs, to enhance repair.
This synergistic approach supports personalized medicine strategies and may reduce the incidence of non-union by enabling timely therapeutic adjustments.
Future Directions and Personalized Medicine
Research is increasingly focused on discovering novel biomarkers and refining analytical techniques such as proteomics, metabolomics, and single-cell transcriptomics. These powerful platforms can uncover previously unrecognized mediators of bone repair and identify patient-specific signatures that predict response to treatment. Emerging interest in exosomal microRNAs and circulating cell-free DNA holds promise for non-invasive monitoring of the molecular landscape during each healing phase.
Advancements in biomaterials and tissue engineering also intersect with biomarker research. Scaffold designs incorporating bioactive molecules aim to deliver growth factors in a controlled manner, enhancing regeneration and structural integrity. Meanwhile, machine learning algorithms analyze complex biomarker datasets alongside clinical and imaging parameters to generate predictive models of healing outcomes. Such integrative frameworks may revolutionize the prognosis and management of bone injuries.
Challenges and Considerations
Despite significant progress, several hurdles remain. Standardizing biomarker assays across laboratories and establishing universally accepted reference ranges are critical for broad clinical adoption. Ethical considerations around personalized data and the cost-effectiveness of advanced multiplex platforms must also be addressed. Moreover, variations in patient demographics, comorbidities, and medication use can influence biomarker levels, requiring careful interpretation within the clinical context.